Obesity and CVD
Defining CMR - Epidemiology - Abdominal Obesity vs. CVD: Beyond Body WeightKey Points
- Obesity is a key determinant of CVD. When compared to normal weight individuals, obese patients have several metabolic complications that increase their CVD risk.
- Although much epidemiological evidence has shown that obesity is a major CVD risk factor, not all obese individuals are at increased risk of CVD.
- Because of the differences observed among obese individuals, special attention must be paid to body fat distribution and to abdominal adipose tissue accumulation in particular, which usually worsens the metabolic profile of overweight/obese patients.
Obesity: a Worldwide Epidemic
It is an established fact that overweight and obesity constitute major public health challenges in today’s society [1]. The number of individuals who are overweight or obese is increasing rapidly, and the World Health Organization (WHO) has gone so far as to call the worldwide rise in obesity a global epidemic [2]. According to the National Health and Nutrition Examination Survey (NHANES III) [3], more than 64% of American adults are overweight and 23% are obese. Unfortunately, this dramatic increase in obesity is not limited to adults. The number of overweight and obese children and adolescents is also on the rise [4]. The increasing prevalence of childhood obesity is a major concern not only because of the short-term health problems it causes, but also because it increases the risk of developing cardiovascular disease (CVD) in adulthood [5].
Obesity: a Key Modifiable Risk Factor for CVD
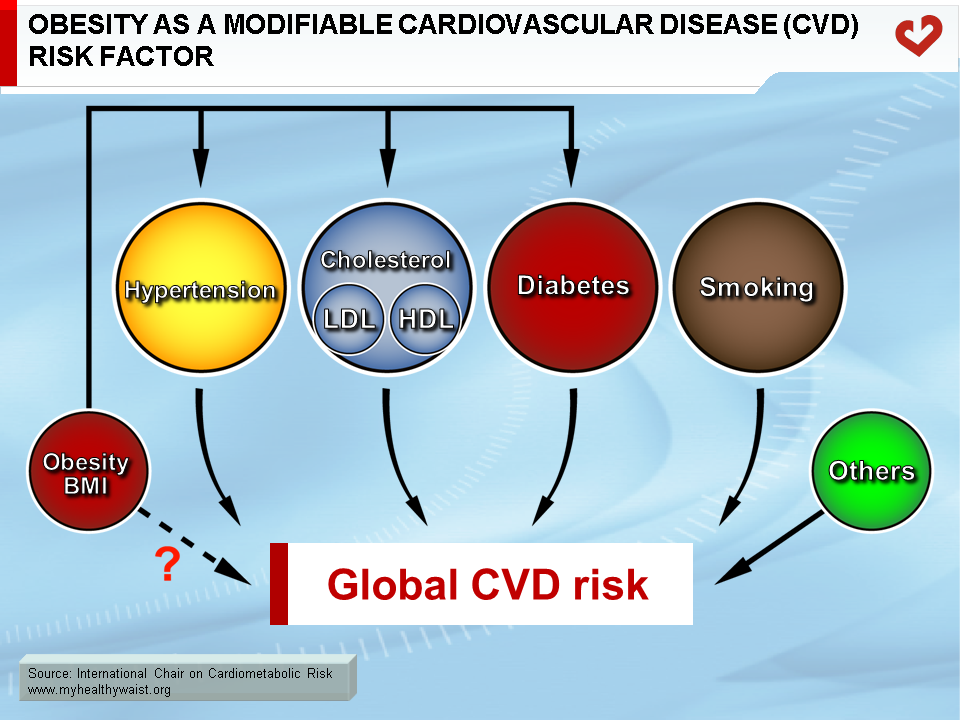
Obesity is a chronic metabolic disorder associated with CVD and increased morbidity and mortality [6-9]. Increased body fat is also associated with numerous co-morbidities such as heart disease, type 2 diabetes, stroke, hypertension, dyslipidemia, certain cancers, and sleep apnea [10]. In clinical practice, however, physicians are continually challenged by the absence of metabolic abnormalities in some obese patients who have a “normal” metabolic profile despite their excess body fat. Because of this, obesity was long not considered among the “heavyweights” of modifiable CVD risk factors, such as smoking, diabetes, a dyslipidemic state, and hypertension (Figure). In addition, there is no independent association between excess body fat and CVD once the relationship between obesity and hypertension, dyslipidemia and diabetes is taken into account. The absence of an independent association between obesity and CVD could be explained by the fact that obesity is heterogeneous as a CVD risk factor.
When the high-risk form of obesity (abdominal obesity) is considered, its impact on CVD could be approximately equal to that of smoking and may even exceed that of LDL cholesterol [11]. It has been suggested that any decrease in smoking-related CVD risk has been offset by the increase in obesity [12]. In this regard, Mokdad et al. [13] have reported that, if obesity rates continue to skyrocket in the next few years, overweight and obesity caused by poor eating habits and physical inactivity will likely overtake tobacco as the leading preventable cause of mortality. In fact, they estimate that about 365,000 deaths annually are due to sedentary lifestyles and poor nutrition. Unfortunately, the sharp rise in overweight and obesity strongly suggests that this number will increase considerably in the near future. In response, the American Heart Association has reclassified obesity as a major modifiable risk factor for coronary heart disease (CHD) [14].
The association between overweight and CVD risk was first recognized in the Framingham Heart Study [15]. After 26 years of follow-up, the study authors concluded that obesity was a significant independent predictor of CVD, including CHD, coronary death, and congestive heart failure in both middle-aged men and women. This relationship was independent of age, cholesterol, systolic blood pressure, cigarette smoking, left ventricular hypertrophy, and glucose intolerance. In addition, when examining the 44 years of Framingham Heart Study follow-up, Wilson et al. [9] showed that CVD risk was higher among overweight and obese men and women after adjusting for age, smoking, high blood pressure, high cholesterol, and diabetes. Moreover, the Nurses’ Health Study [16]—a 16-year follow-up study—indicated that the risk of death from CVD was significantly higher among overweight and obese women (body mass index (BMI)>27 kg/m2) as compared to lean women (BMI<19 kg/m2). Overweight and obesity must therefore be considered significant and hopefully modifiable CVD risk factors.
In another study examining obesity’s contribution to CVD risk, Mora et al. [17] demonstrated that a high BMI value significantly increased CHD risk in apparently healthy siblings from families with premature CHD, but mainly among siblings with a high Framingham risk score. Significantly, adiposity indices such as BMI were not initially included in the Framingham risk score, which uses sex-specific risk equations to estimate CHD events based on variables such as age, total cholesterol, HDL cholesterol, blood pressure, diabetes, and smoking status [18]. Mora et al. [17] have also demonstrated that BMI is an independent predictor of CHD risk that lends additional predictive weight to the Framingham risk score. Moreover, normal weight subjects with an elevated Framingham risk score were shown to have a low CHD event rate similar to normal weight subjects with a low Framingham risk score. Thus, it appears that the landscape of modifiable CVD risk factors has evolved over the last 50 years and that obesity is now a major cause of CVD. In this regard, the Framingham Heart Study now includes BMI as a predictor of 10-year CVD risk [19] and 30-year CVD risk [20] in their algorithms using non-laboratory-based predictors. Several risk functions are available on the Framingham Heart Study website.
Obesity: the Primary Cause of The Metabolic Syndrome?
The metabolic syndrome is a cluster of metabolic complications—including atherogenic dyslipidemia, insulin resistance, glucose intolerance, raised blood pressure, and a prothrombotic and inflammatory state—that are more often found in patients with abdominal obesity [21]. As a common metabolic disorder, the metabolic syndrome is directly linked to obesity, abdominal obesity in particular [21]. Because of the syndrome’s ties to obesity, the number of individuals with the metabolic syndrome has risen in step with the worldwide obesity and diabetes epidemic [22]. This rise in obesity has facilitated recognition of the syndrome and, consequently, the importance of abdominal obesity as a key contributor to the metabolic syndrome. The recent inclusion of waist circumference as a clinical criterion for diagnosing the metabolic syndrome [23] cements the key role played by abdominal obesity in the metabolic syndrome [24]. Therefore, in addition to overweight and obesity—both established risk factors for the metabolic syndrome—patterns of body fat distribution (i.e., abdominal obesity) may increase risk for this diabetogenic and atherogenic condition [25].
References
-
Bray GA, Bouchard C and James WPT, eds. Handbook of obesity. New York: Marcel Dekker. 1998.
PubMed ID:
-
WHO 2000 Obesity: Preventing and managing the global epidemic. Report of a WHO consultation. [WHO Technical report series No. 894]. Geneva. World Health Organization 2000.
PubMed ID:
-
Kuczmarski RJ, Flegal KM, Campbell SM, et al. Increasing prevalence of overweight among US adults. The National Health and Nutrition Examination Surveys, 1960 to 1991. JAMA 1994; 272: 205-11.
PubMed ID: 8022039
-
Engeland A, Bjorge T, Sogaard AJ, et al. Body mass index in adolescence in relation to total mortality: 32-year follow-up of 227,000 Norwegian boys and girls. Am J Epidemiol 2003; 157: 517-23.
PubMed ID: 12631541
-
Krauss RM, Winston M, Fletcher BJ, et al. Obesity: impact on cardiovascular disease. Circulation 1998; 98: 1472-6.
PubMed ID: 9760304
-
Drenick EJ, Bale GS, Seltzer F, et al. Excessive mortality and causes of death in morbidly obese men. JAMA 1980; 243: 443-5.
PubMed ID: 7351764
-
Manson JE, Willett WC, Stampfer MJ, et al. Body weight and mortality among women. N Engl J Med 1995; 333: 677-85.
PubMed ID: 7637744
-
Willett WC, Manson JE, Stampfer MJ, et al. Weight, weight change, and coronary heart disease in women. Risk within the ‘normal’ weight range. JAMA 1995; 273: 461-5.
PubMed ID: 7654270
-
Wilson PW, D’Agostino RB, Sullivan L, et al. Overweight and obesity as determinants of cardiovascular risk: the Framingham experience. Arch Intern Med 2002; 162: 1867-72.
PubMed ID: 12196085
-
Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults–The Evidence Report. National Institutes of Health. Obes Res 1998; 6 Suppl 2: 51S-209S.
PubMed ID: 9813653
-
Allison DB, Fontaine KR, Manson JE, et al. Annual deaths attributable to obesity in the United States. JAMA 1999; 282: 1530-8.
PubMed ID: 10546692
-
Hu FB, Stampfer MJ, Manson JE, et al. Trends in the incidence of coronary heart disease and changes in diet and lifestyle in women. N Engl J Med 2000; 343: 530-7.
PubMed ID: 10954760
-
Mokdad AH, Marks JS, Stroup DF, et al. Actual causes of death in the United States, 2000. JAMA 2004; 291: 1238-45.
PubMed ID: 15010446
-
Eckel RH and Krauss RM. American Heart Association call to action: obesity as a major risk factor for coronary heart disease. AHA Nutrition Committee. Circulation 1998; 97: 2099-100.
PubMed ID: 9626167
-
Hubert HB, Feinleib M, McNamara PM, et al. Obesity as an independent risk factor for cardiovascular disease: a 26- year follow-up of participants in the Framingham Heart Study. Circulation 1983; 67: 968-77.
PubMed ID: 6219830
-
Manson JE, Colditz GA, Stampfer MJ, et al. A prospective study of obesity and risk of coronary heart disease in women. N Engl J Med 1990; 322: 882-9.
PubMed ID: 2314422
-
Mora S, Yanek LR, Moy TF, et al. Interaction of body mass index and framingham risk score in predicting incident coronary disease in families. Circulation 2005; 111: 1871-6.
PubMed ID: 15837938
-
Wilson PW, D’Agostino RB, Levy D, et al. Prediction of coronary heart disease using risk factor categories. Circulation 1998; 97: 1837-47.
PubMed ID: 9603539
-
D’agostino RB, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care. Circulation 2008; 117: 743-53.
PubMed ID: 18212285
-
Pencina MJ, D’Agostino Sr RB, Larson MG, et al. Predicting the thirty-year risk of cardiovascular disease: the Framingham Heart Study. Circulation 2009; 119: 3078-84.
PubMed ID: 19506114
-
Eckel RH, Grundy SM and Zimmet PZ. The metabolic syndrome. Lancet 2005; 365: 1415-28.
PubMed ID: 15836891
-
Zimmet P, Alberti KG and Shaw J. Global and societal implications of the diabetes epidemic. Nature 2001; 414: 782-7.
PubMed ID: 11742409
-
Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001; 285: 2486-97.
PubMed ID: 11368702
-
Després JP and Lemieux I. Abdominal obesity and metabolic syndrome. Nature 2006; 444: 881-7.
PubMed ID: 17167477
-
Després JP, Nadeau A, Tremblay A, et al. Role of deep abdominal fat in the association between regional adipose tissue distribution and glucose tolerance in obese women. Diabetes 1989; 38: 304-9.
PubMed ID: 2645187
 CLOSE
CLOSE
CLOSE
CLOSE
CLOSE
CLOSE
Kuczmarski RJ, Flegal KM, Campbell SM, et al. Increasing prevalence of overweight among US adults. The National Health and Nutrition Examination Surveys, 1960 to 1991. JAMA 1994; 272: 205-11.
PubMed ID: 8022039CLOSE
Engeland A, Bjorge T, Sogaard AJ, et al. Body mass index in adolescence in relation to total mortality: 32-year follow-up of 227,000 Norwegian boys and girls. Am J Epidemiol 2003; 157: 517-23.
PubMed ID: 12631541CLOSE
Krauss RM, Winston M, Fletcher BJ, et al. Obesity: impact on cardiovascular disease. Circulation 1998; 98: 1472-6.
PubMed ID: 9760304CLOSE
Drenick EJ, Bale GS, Seltzer F, et al. Excessive mortality and causes of death in morbidly obese men. JAMA 1980; 243: 443-5.
PubMed ID: 7351764CLOSE
Manson JE, Willett WC, Stampfer MJ, et al. Body weight and mortality among women. N Engl J Med 1995; 333: 677-85.
PubMed ID: 7637744CLOSE
Willett WC, Manson JE, Stampfer MJ, et al. Weight, weight change, and coronary heart disease in women. Risk within the ‘normal’ weight range. JAMA 1995; 273: 461-5.
PubMed ID: 7654270CLOSE
Wilson PW, D’Agostino RB, Sullivan L, et al. Overweight and obesity as determinants of cardiovascular risk: the Framingham experience. Arch Intern Med 2002; 162: 1867-72.
PubMed ID: 12196085CLOSE
Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults–The Evidence Report. National Institutes of Health. Obes Res 1998; 6 Suppl 2: 51S-209S.
PubMed ID: 9813653CLOSE
Allison DB, Fontaine KR, Manson JE, et al. Annual deaths attributable to obesity in the United States. JAMA 1999; 282: 1530-8.
PubMed ID: 10546692CLOSE
Hu FB, Stampfer MJ, Manson JE, et al. Trends in the incidence of coronary heart disease and changes in diet and lifestyle in women. N Engl J Med 2000; 343: 530-7.
PubMed ID: 10954760CLOSE
Mokdad AH, Marks JS, Stroup DF, et al. Actual causes of death in the United States, 2000. JAMA 2004; 291: 1238-45.
PubMed ID: 15010446CLOSE
Eckel RH and Krauss RM. American Heart Association call to action: obesity as a major risk factor for coronary heart disease. AHA Nutrition Committee. Circulation 1998; 97: 2099-100.
PubMed ID: 9626167CLOSE
Hubert HB, Feinleib M, McNamara PM, et al. Obesity as an independent risk factor for cardiovascular disease: a 26- year follow-up of participants in the Framingham Heart Study. Circulation 1983; 67: 968-77.
PubMed ID: 6219830CLOSE
Manson JE, Colditz GA, Stampfer MJ, et al. A prospective study of obesity and risk of coronary heart disease in women. N Engl J Med 1990; 322: 882-9.
PubMed ID: 2314422CLOSE
Mora S, Yanek LR, Moy TF, et al. Interaction of body mass index and framingham risk score in predicting incident coronary disease in families. Circulation 2005; 111: 1871-6.
PubMed ID: 15837938CLOSE
Wilson PW, D’Agostino RB, Levy D, et al. Prediction of coronary heart disease using risk factor categories. Circulation 1998; 97: 1837-47.
PubMed ID: 9603539CLOSE
D’agostino RB, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care. Circulation 2008; 117: 743-53.
PubMed ID: 18212285CLOSE
Pencina MJ, D’Agostino Sr RB, Larson MG, et al. Predicting the thirty-year risk of cardiovascular disease: the Framingham Heart Study. Circulation 2009; 119: 3078-84.
PubMed ID: 19506114CLOSE
Eckel RH, Grundy SM and Zimmet PZ. The metabolic syndrome. Lancet 2005; 365: 1415-28.
PubMed ID: 15836891CLOSE
Zimmet P, Alberti KG and Shaw J. Global and societal implications of the diabetes epidemic. Nature 2001; 414: 782-7.
PubMed ID: 11742409CLOSE
Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001; 285: 2486-97.
PubMed ID: 11368702CLOSE
Després JP and Lemieux I. Abdominal obesity and metabolic syndrome. Nature 2006; 444: 881-7.
PubMed ID: 17167477CLOSE
Després JP, Nadeau A, Tremblay A, et al. Role of deep abdominal fat in the association between regional adipose tissue distribution and glucose tolerance in obese women. Diabetes 1989; 38: 304-9.
PubMed ID: 2645187