

Laboratoire d'Études Moléculaires des Valvulopathies (LEMV); Groupe de Recherche en Valvulopathies (GRV); Hôpital Laval Research Centre/Quebec Heart Institute; Department of Surgery, Université Laval, Quebec City, Quebec, Canada.
patrick.mathieu@chg.ulaval.ca
philippe.pibarot@med.ulaval.ca
jean-pierre.despres@crhl.ulaval.ca

 [Click to enlarge]
[Click to enlarge]
Visceral obesity has been recognized in recent years as a strong determinant of metabolic abnormalities and cardiovascular risk [1]. In the last decade, we have also seen an increasing number of individuals with visceral obesity, insulin resistance and the atherogenic lipoprotein phenotype [2]. More and more studies have highlighted the fact that excess abdominal fat is the strongest determinant of metabolic disorders [3]. These studies have helped to single out important components associated with visceral obesity, such as low HDL concentrations, high triglyceride levels, insulin resistance and a low-grade inflammatory state [4]. While these metabolic disorders have been established as important determinants of coronary events, it is only recently that these abnormalities associated with visceral obesity have been evaluated as potential risk factors following heart surgery [5]. In addition to playing a role in atherosclerosis, at-risk abdominal obesity is also thought to play a role in the degeneration of implanted valve bioprostheses (BPs) [6]. Hence, it now appears that visceral obesity is a global cardiovascular risk that also encompasses surgical risk and heart valve diseases.
The metabolic syndrome: a risk factor in cardiac surgery
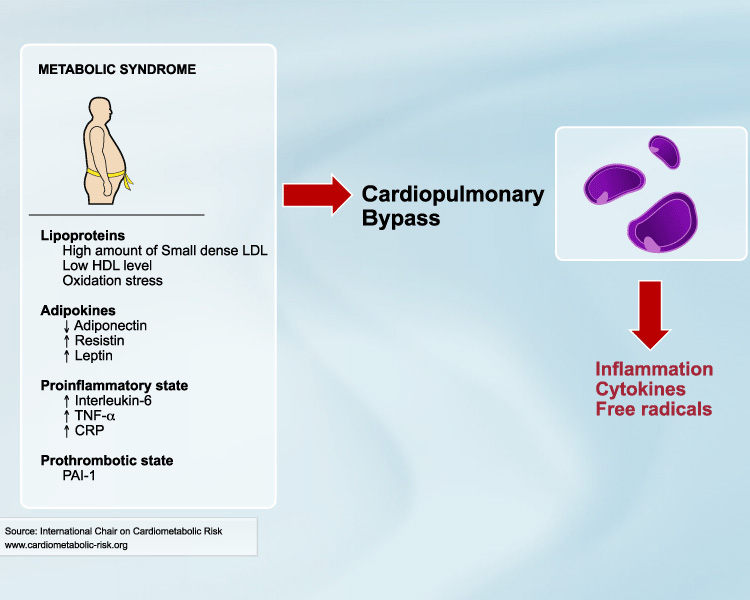
In previous studies, diabetes has been associated with increased morbidity following a cardiac surgery [7]. However, whether diabetes increases perioperative mortality is contentious [8, 9]. Furthermore, while obesity, as defined by body mass index (BMI), has been associated with increased morbidity following a coronary artery bypass grafting (CABG) surgery, it has not been associated with a higher mortality rate [10]. In light of the pro-inflammatory condition associated with abdominal obesity, we have recently hypothesized that individuals characterized by the metabolic syndrome (MS) would be at greater risk. In 5,304 patients undergoing a CABG, we documented that a substantial proportion of patients (46%) were characterized by the MS.
 [Click to enlarge]
[Click to enlarge]
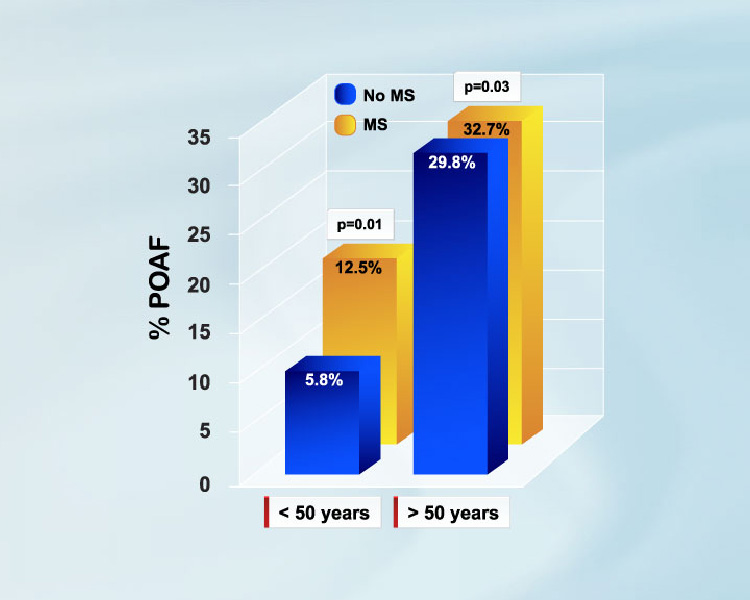
We also found that the MS conferred a three-fold risk of in-hospital mortality and was independently associated with postoperative complications such as renal failure and atrial fibrillation (AF) [5, 11]. Significantly, subjects with diabetes and without the MS were not at higher risk. Although the mechanisms underpinning these processes are complex and not yet fully understood, it is tempting to speculate that low grade inflammation associated with visceral obesity could increase in the postoperative period, contributing to the development of complications.
Postoperative AF, a common complication following cardiac surgery with incidence varying between 30-50%, is associated with a substantial increase in morbidity and cost for the healthcare system [12]. The mechanisms that contribute to this arrhythmia in the postoperative period are multifaceted and may involve oxidative stress as well as activation of the autonomic system [13]. In addition, obese individuals have a higher prevalence of ventricular diastolic dysfunction and elevated plasma volume, which may contribute to atrial remodelling [14]. Atrial remodelling and enlargement may therefore provide an anatomical substrate by which triggering factors in the postoperative period can cause electrical inhomogeneity and arrhythmia.
Given the high prevalence of the MS in the surgical population referred to CABG, the large number of procedures performed each year worldwide and the three-fold risk of operative mortality conferred by the MS, reducing the prevalence of this condition would certainly lead to better outcomes. However, the question remains as to whether the operative risk associated with the MS could be modified in the context of emergent non-elective procedures. In order to resolve this issue, further research is needed to identify the mechanisms associated with the MS and surgical mortality/morbidity and thereby fuel the development of novel therapeutic strategies to acutely reduce this risk.
Is structural degeneration of bioprostheses an atherosclerotic process?
Patients with advanced heart valve diseases often require valve replacement with prostheses. Currently, some 275,000 valve replacements are performed each year worldwide. It is estimated that bioprotheses (BPs) are used in half of these procedures. The use of a BP has the major advantage of obviating the need for anticoagulation in individuals for whom there is no other clinical indication of such treatment. However, the long-term longevity of BPs is impeded by structural valve degeneration (SVD), a process related to calcification and destruction of the extra-cellular matrix [15]. For years, SVD of BPs has been thought of as a passive process in which chemical fixation of tissues before implantation was responsible for calcification and subsequent degeneration, leading to clinical failure years after implantation. In recent years, different studies have identified that hypercholesterolemia, diabetes and absence of statin therapy were independent risk factors for the occurrence of BP dysfunction [6]. More recently, Briand et al. [6] have documented that diabetes, renal insufficiency and the MS were independent risk factors for the development of hemodynamic dysfunction of BPs. These studies have helped to highlight that SVD could be an active process that is influenced by atherosclerotic risk factors in the postoperative period.
 [Click to enlarge]
[Click to enlarge]
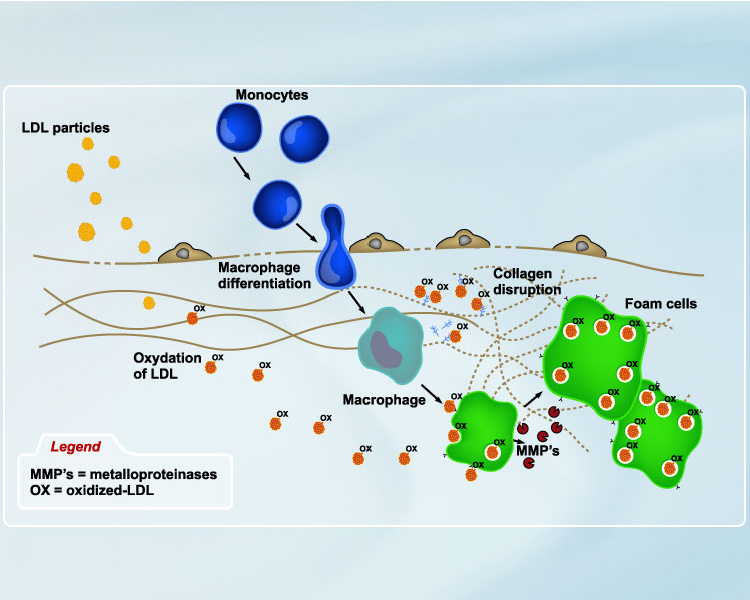
Examination of explanted BPs has revealed that many prostheses have significant amounts of accumulated lipids. We recently demonstrated that most of these lipids were oxidized-LDLs (oxLDLs) and were located in areas of low shear stress. Moreover, oxLDLs were colocalized with dense cellular infiltrates composed of macrophages. Of particular significance is the fact that foam cells were identified along with macrophages expressing scavenger receptors. Furthermore, activated macrophages expressed a high level of metalloproteinase-9 (MMP-9) and could thus play a role in matrix degradation. These studies strengthened the hypothesis that a lipid-driven process, which could be influenced by metabolic factors, participates in the SVD process. Hence, recent clinical and pathological studies have underlined that modifiable risk factors contribute to SVD and may thus represent new, near-term therapeutic avenues in order to promote the longevity of implanted BPs.
Conclusion
Recent studies have identified that the MS is a frequent condition in those who undergo heart surgery and that it is independently associated with a substantial operative risk. Furthermore, metabolic risk factors have been shown to influence the development of heart valve diseases, including SVD of BPs. Emerging evidence indicates that visceral obesity must be considered a global cardiovascular risk that acts at multiple levels, from the development of coronary artery disease and heart valve pathology to the operative risk associated with CABG. It is thus of crucial importance to reduce the prevalence of at-risk obesity and develop efficient therapeutic strategies for individuals with this risk factor.
References
- Després JP and Lemieux I. Abdominal obesity and metabolic syndrome. Nature 2006; 444: 881-7.
- Lamarche B, Lemieux I and Després JP. The small, dense LDL phenotype and the risk of coronary heart disease: epidemiology, patho-physiology and therapeutic aspects. Diabetes Metab 1999; 25: 199-211.
- St-Pierre J, Lemieux I, Vohl MC, et al. Contribution of abdominal obesity and hypertriglyceridemia to impaired fasting glucose and coronary artery disease. Am J Cardiol 2002; 90: 15-8.
- Després JP, Lemieux I, Dagenais GR, et al. Evaluation and management of atherogenic dyslipidemia: beyond low-density lipoprotein cholesterol. CMAJ 2001; 165: 1331-3.
- Echahidi N, Pibarot P, Després JP, et al. Metabolic syndrome increases operative mortality in patients undergoing coronary artery bypass grafting surgery. J Am Coll Cardiol 2007; 50: 843-51.
- Briand M, Pibarot P, Després JP, et al. Metabolic syndrome is associated with faster degeneration of bioprosthetic valves. Circulation 2006; 114: I512-7.
- Brandt M, Harder K, Walluscheck KP, et al. Coronary artery bypass surgery in diabetic patients. J Card Surg 2004; 19: 36-40.
- Carson JL, Scholz PM, Chen AY, et al. Diabetes mellitus increases short-term mortality and morbidity in patients undergoing coronary artery bypass graft surgery. J Am Coll Cardiol 2002; 40: 418-23.
- Nalysnyk L, Fahrbach K, Reynolds MW, et al. Adverse events in coronary artery bypass graft (CABG) trials: a systematic review and analysis. Heart 2003; 89: 767-72.
- Zacharias A, Schwann TA, Riordan CJ, et al. Obesity and risk of new-onset atrial fibrillation after cardiac surgery. Circulation 2005; 112: 3247-55.
- Echahidi N, Mohty D, Pibarot P, et al. Obesity and metabolic syndrome are independent risk factors for atrial fibrillation after coronary artery bypass graft surgery. Circulation 2007; 116: I213-9.
- Almassi GH, Schowalter T, Nicolosi AC, et al. Atrial fibrillation after cardiac surgery: a major morbid event? Ann Surg 1997; 226: 501-11.
- Ceriello A and Motz E. Is oxidative stress the pathogenic mechanism underlying insulin resistance, diabetes, and cardiovascular disease? The common soil hypothesis revisited. Arterioscler Thromb Vasc Biol 2004; 24: 816-23.
- Iacobellis G, Ribaudo MC, Leto G, et al. Influence of excess fat on cardiac morphology and function: study in uncomplicated obesity. Obes Res 2002; 10: 767-73.
- Schoen FJ. Future directions in tissue heart valves: impact of recent insights from biology and pathology. J Heart Valve Dis 1999; 8: 350-8.
