

Groupe de Recherche en Valvulopathies (GRV),
Hôpital Laval Research Centre / Quebec Heart Institute Université Laval, Quebec, Canada
philippe.pibarot@med.ulaval.ca

Valvulo-metabolic risk can be defined as the risk of valvular heart disease resulting from the metabolic abnormalities associated with visceral obesity and the metabolic syndrome (MS). It is therefore he cardiometabolic risk that specifically relates to valvular heart disease.
Burden of aortic valve stenosis
Calcific aortic valve disease starts with a thickening and calcification of the aortic valve cusps, named aortic valve sclerosis, which subsequently progresses toward aortic valve stenosis (AS) causing significant hemodynamic obstruction of the left ventricular (LV) outflow tract. Calcific AS is the most frequent cardiovascular disease after coronary artery disease (CAD) and hypertension in developed countries. The prevalence of AS in the USA is 0.3-0.5%, which translates to approximately 600,000 to 1 million people. The prevalence of AS also increases markedly with age: from 0.02% in 18-44 year olds to 3.0 % in the 75 years and older group. It is projected that 40% of people over age 65 are expected to survive to age 90 in the year 2050 compared to 25% in 2000. This major increase in life expectancy during the next several decades will increase the burden of valvular heart diseases. The only efficient treatment for symptomatic severe AS is aortic valve replacement surgery or transcatheter valve implantation. It is estimated that AS is directly responsible for approximately 15,000 deaths and 80,000 valve procedures per year in North America. This disease is therefore associated with a major health and socio-economic burden.
Aortic valve stenosis: an atherosclerotic disease?
For a long time, calcific AS has been considered a "degenerative" disease because it was thought to be the result of aging and "wear and tear" of the aortic valve. This perception has changed over the years with the publication of several studies showing that AS shares many cellular similarities with vascular atherosclerosis. Furthermore, AS has been linked to several traditional risk factors for CAD including age, male gender, hypercholesterolemia, diabetes, hypertension, smoking, and obesity. There is now a growing body of evidence supporting the concept that AS is an active disease involving atherosclerotic pathways. This, in turn, raises the possibility that AS might be a modifiable disease. However, we cannot directly transpose what we have learned about CAD or peripheral arterial disease to aortic valve disease because there are important anatomical and biomechanical distinctions between the aortic valve and the arteries. Moreover, the occurrence of clinical events is essentially determined by plaque vulnerability (inflammation, large lipid core, thin fibrous cap) in CAD versus volume and stiffness of aortic valve cups in AS. Hence, calcification is a predominant factor in aortic valve disease, whereas its role in CAD remains unclear.
Valvulo-metabolic risk in aortic stenosis
 [Click to enlarge]
[Click to enlarge]
 [Click to enlarge]
[Click to enlarge]
The team of Drs. Couet and Arsenault at Hôpital Laval Research Centre induced visceral obesity and some typical features of the MS by feeding a wild-type mouse strain with a high carbohydrate/high fat diet [1]. Interestingly, these animals developed a mild aortic valve stenosis over a period of four months. These experimental data prompted us to examine the association between the MS and progression of aortic valve disease in patients with at least moderate AS [2]. In this population, 40% of the patients had the NCEP-ATP III clinical criteria of the MS. The patients with the MS had a much faster stenosis progression as documented by Doppler-echocardiography and a four-fold increase in the risk of adverse events defined as aortic valve replacement or death (Figure 1) [2].
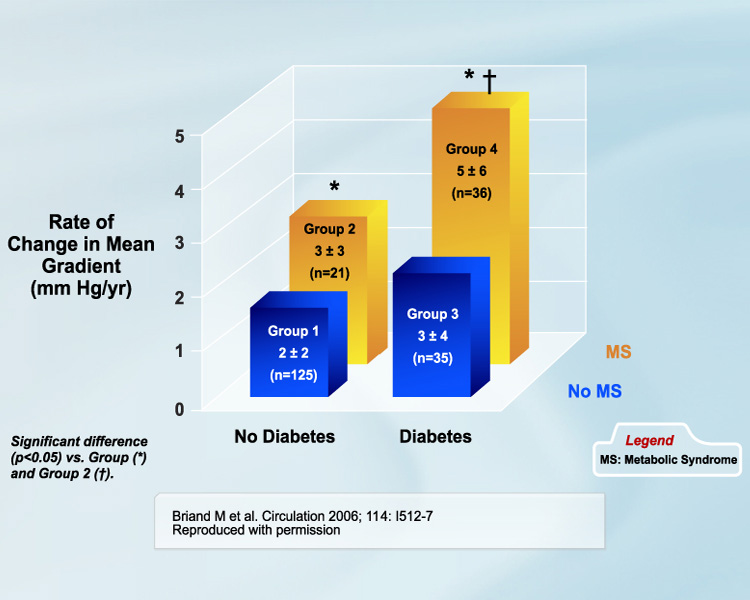
These results are also consistent with those of the large epidemiological study Multi- Ethnic Study of Atherosclerosis (MESA), where the prevalence of aortic valve sclerosis was markedly higher in the subjects with the MS and/or diabetes [3]. This association was observed in both men and women. We also found that valvulo-metabolic risk may persist beyond aortic valve replacement. The diseased native valve is often replaced by a bioprosthetic valve made of bovine or porcine tissues fixed with glutaraldehyde. The "Achilles heel" of these bioprostheses is their limited durability. The bioprosthetic tissue may indeed undergo degenerative processes leading to valve stenosis or regurgitation; these processes are more frequent and faster in younger patients. We recently reported that the MS and diabetes are powerful independent predictors of the degeneration of bioprosthetic valves (Figure 2) [4]. These provocative results suggest that, in contrast to previous beliefs, some active mechanisms potentially related to atherosclerotic pathways may contribute to the structural deterioration of bioprosthetic valves.
 [Click to enlarge]
[Click to enlarge]
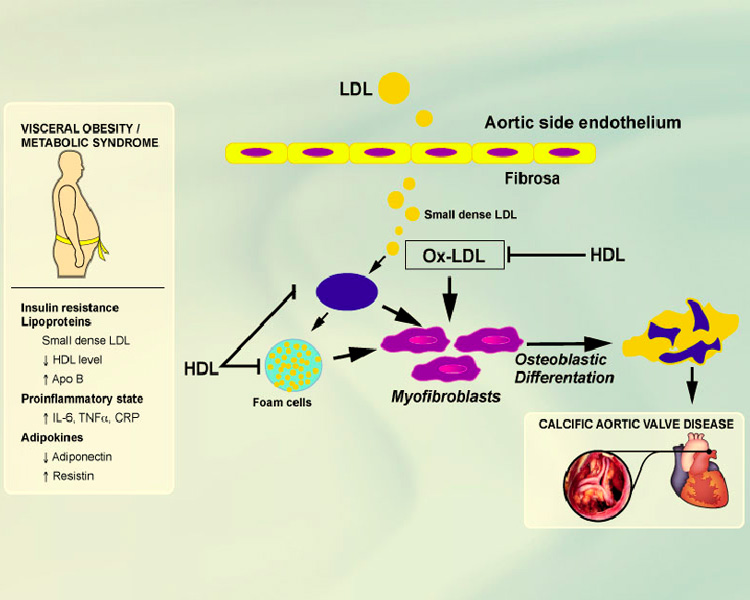
Figure 3 presents the factors that may explain the association between the MS and calcific aortic valve disease of both native and bioprosthetic valves. Visceral obesity, which is by far the most prevalent form of the MS, is associated with enhanced production of small dense LDL particles; reduced plasma levels of HDL; increased production of inflammatory cytokines such as interleukin-6, tumor necrosis factor-α, and C-reactive protein; and reduced production of the "good" adipokine, adiponectin, which has several anti-atherogenic properties. These factors may enhance production of oxidized LDL and may stimulate inflammation and osteoblastic differentiation of myofibroblasts within the aortic valve cusps. When analyzed collectively, these findings suggest that the metabolic abnormalities associated with visceral obesity and the metabolic syndrome may be involved in the development and progression of native aortic valve disease and with the structural deterioration of the bioprosthetic valve following aortic valve replacement.
Implications with regard to prevention and treatment of aortic stenosis
In light of these findings, patients diagnosed with aortic valve sclerosis or stenosis or who underwent bioprosthetic valve implantation should be systematically screened for the presence of the MS (using the hypertriglyceridemic waist, NCEP-ATP III, or IDF algorithms). If the MS is present, these patients should probably be followed more closely so as to track the evolution of their valve function and the appearance of symptoms. Aggressive changes in lifestyle habits, such as increasing physical activity and implementing dietary changes to reduce waist circumference, should also be applied in these high risk patients. However, targeting the features of the MS with some specific pharmacological approach should be withheld until the benefit of such medications is established in clinical trials.
 [Click to enlarge]
[Click to enlarge]
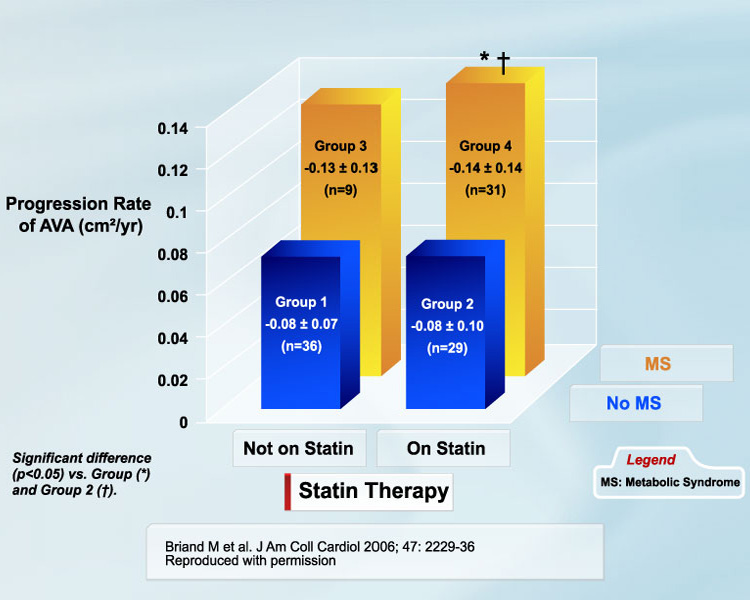
The two pharmacological agents that are currently under the most scrutiny for potentially delaying AS progression are statins and ACE inhibitors. The two first clinical trials published until now have provided conflicting results [5, 6]. The SLATIRE trial showed no significant difference between the statin and the placebo with regard to stenosis progression [5], whereas the open-label RAAVE trial reported a slower stenosis progression in patients with elevated LDL treated with statin compared to those with normal LDL left untreated [6]. When analyzed collectively, these studies suggest that AS patients with hypercholesterolemia may benefit from statin therapy and that these drugs may be more efficient in the early stages (i.e., aortic valve sclerosis or mild/moderate AS) than in the late stages (i.e., severe AS) of the disease. However, it is well known that statins and ACE inhibitors have little or no effect on the metabolic perturbations associated with the MS. As a matter of fact, in our recent study, we found that patients with the MS had a fast stenosis progression and a high risk of adverse events, regardless of the presence of statin therapy (Figure 4).
These findings further support the concept that statins may be necessary but not sufficient in a substantial proportion of patients, those with the MS in particular, and that other targets of therapy should be considered in these patients. The findings presented in this article suggest that visceral obesity may be a promising therapeutic target in those with calcific aortic valve disease. To this end, we need properly designed mechanistic and interventional studies to determine the most appropriate behavioural or pharmacological approaches to efficiently reduce and manage valvulo-metabolic risk.
References
- Drolet MC, Roussel E, Deshaies Y, et al. A high fat/high carbohydrate diet induces aortic valve disease in C57BL/6J mice. J Am Coll Cardiol 2006; 47: 850-5.
- Briand M, Lemieux I, Dumesnil JG, et al. Metabolic syndrome negatively influences disease progression and prognosis in aortic stenosis. J Am Coll Cardiol 2006; 47: 2229-36.
- Katz R, Wong ND, Kronmal R, et al. Features of the metabolic syndrome and diabetes mellitus as predictors of aortic valve calcification in the Multi-Ethnic Study of Atherosclerosis. Circulation 2006; 113: 2113-9.
- Briand M, Pibarot P, Després JP, et al. Metabolic syndrome is associated with faster degeneration of bioprosthetic valves. Circulation 2006; 114: I512-7.
- Cowell SJ, Newby DE, Prescott RJ, et al. A randomized trial of intensive lipid-lowering therapy in calcific aortic stenosis. N Engl J Med 2005; 352: 2389-97.
- Moura LM, Ramos SF, Zamorano JL, et al. Rosuvastatin affecting aortic valve endothelium to slow the progression of aortic stenosis. J Am Coll Cardiol 2007; 49: 554-61.
