CVD risk and type 2 diabetes: Beyond hyperglycemia
Defining CMR - Epidemiology - Type 2 DiabetesKey Points
- Type 2 diabetes is a significant CVD risk factor. However, the independent contribution of hyperglycemia per se to CVD risk remains uncertain.
- The hyperglycemic state of diabetes is only one of the dysmetabolic components observed in patients, who are often abdominally obese.
- The cluster of atherogenic metabolic abnormalities now often referred to as the metabolic syndrome is known to increase the risk of type 2 diabetes and CVD.
- Intervention trials have shown that reducing body weight in overweight and obese subjects at high risk of developing diabetes could substantially reduce their risk of developing diabetes.
- Age is also an important factor to consider when evaluating the CVD risk of diabetic patients.
Abdominal Obesity
Type 2 diabetes is recognized as a significant cardiovascular disease (CVD) risk factor, but the independent contribution of type 2 diabetic hyperglycemia to CVD risk is rather weak. It has been proposed that this hyperglycemic state is only the tip of a huge dysmetabolic iceberg, mostly resulting from a combination of factors found in overweight and obese patients with excess abdominal fat and insulin resistance [1].
Abdominal obesity is associated with a cluster of atherogenic metabolic abnormalities that are now often referred to as the metabolic syndrome. These abnormalities include atherogenic dyslipidemia, insulin resistance, and a pro-thrombotic and pro-inflammatory state. The simultaneous presence of all these risk factors is known to increase the risk of type 2 diabetes and CVD [2]. At specific fault is excess visceral adipose tissue, which is more closely associated with a detrimental metabolic profile than excess subcutaneous adipose tissue [3]. This observation has led to the widespread use of waist circumference (a surrogate measure of visceral adipose tissue) in epidemiological analyses and as a metabolic syndrome identification criterion [4,5]. In the Insulin Resistance in Atherosclerosis Study (IRAS), high waist circumference predicted the incidence of metabolic syndrome more accurately than directly measured insulin resistance [6]. Moreover, a prospective study has been published on the predictive power of high initial levels of visceral fat as a type 2 diabetes risk factor [7]. Intervention trials have also confirmed the strong association between excess body fat and type 2 diabetes found in observational studies. These trials have shown that reducing body weight in overweight and obese subjects at high risk of developing diabetes could substantially reduce the incidence of diabetes [8-10].
Insulin Resistance
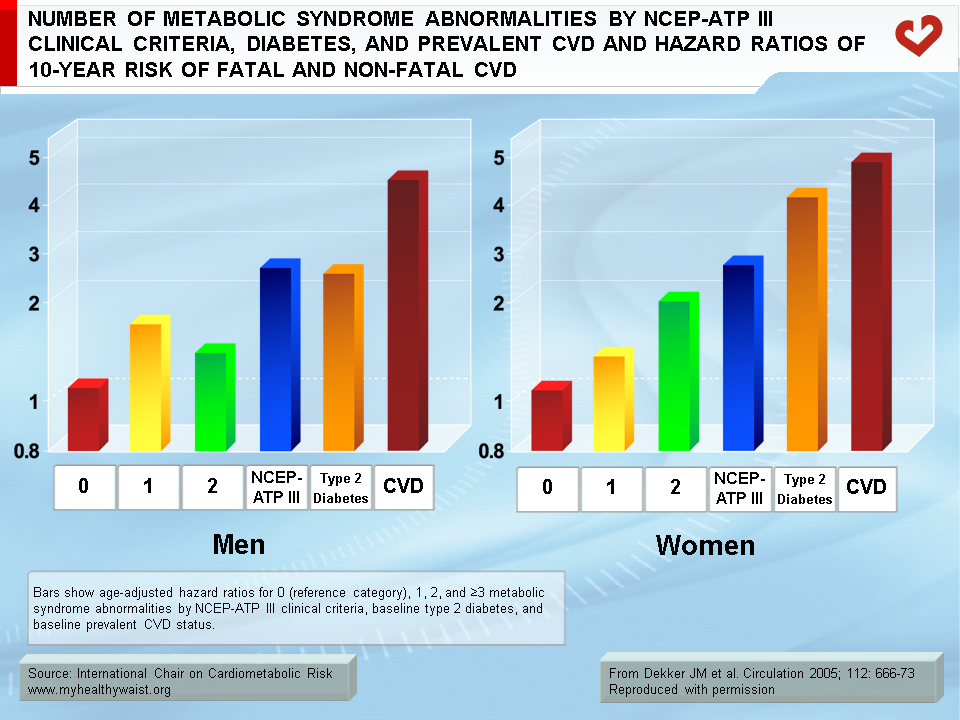
Some investigators argue that it is not the metabolic syndrome that is responsible for increasing CVD risk, but rather insulin resistance state per se [11]. Several clinical criteria and cutoff values have been proposed to identify individuals with the metabolic syndrome and each has a different relationship to insulin resistance. A prospective analysis has demonstrated that insulin resistance substantially increases diabetes or CVD risk in people with the metabolic syndrome, but in the general population, risk prediction in the presence of the metabolic syndrome is similar whether or not insulin resistance is accounted for [12]. The Hoorn study [13] found that the metabolic syndrome increased CVD risk roughly twofold. This study also revealed that men with the metabolic syndrome—according to National Cholesterol Education Program-Adult Treatment Panel III (NCEP-ATP III) clinical criteria—had similar CVD risk as men with diabetes but less risk than men with prevalent CVD (Figure 1). However, metabolic syndrome criteria that included information on fasting insulin levels were no better predictors of CVD risk than those that did not take this insulin resistance marker into account. Similarly, results from the IRAS [14] revealed that there is no need to measure plasma glucose-insulin levels through oral glucose tolerance testing or insulin resistance measures in order to predict diabetes risk. It is sufficient to identify the metabolic syndrome using NCEP-ATP III or International Diabetes Federation (IDF) clinical criteria. In contrast, data from the Framingham Offspring Study [15] revealed that plasma glucose-insulin levels measured after an oral glucose tolerance test could increase CVD risk beyond that of the metabolic syndrome. However, indirect measures of insulin resistance—such as the homeostasis model assessment formula (HOMA-IR) requiring only fasting glucose and insulin measurements—could not improve prediction of diabetes risk.
Dyslipidemia
Besides glucose, various plasma lipid variables also play a role in increasing CVD risk. The regulation of lipoprotein and vascular physiology appears to be related to normal insulin sensitivity. Insulin resistance is associated with the typical dyslipidemic profile seen in patients with type 2 diabetes. This profile is characterized by increased levels of fasting triglycerides, low levels of HDL cholesterol, and elevated concentrations of small, dense LDL, which is the most atherogenic component of LDL cholesterol [16]. Results from a recent study revealed that in coronary patients with type 2 diabetes, the low HDL cholesterol/high triglyceride pattern correlates with the prevalence of coronary artery disease and significantly predicts the incidence of vascular events, but the LDL-related factor does not [17]. It is generally accepted based on data from numerous studies that high triglyceride-low HDL cholesterol dyslipidemia is an independent risk factor for CVD among people with diabetes [18]. Accordingly, three intervention trials have shown improvement in CVD risk with successful treatment of diabetes-related dyslipidemia [19].
Metabolic Syndrome
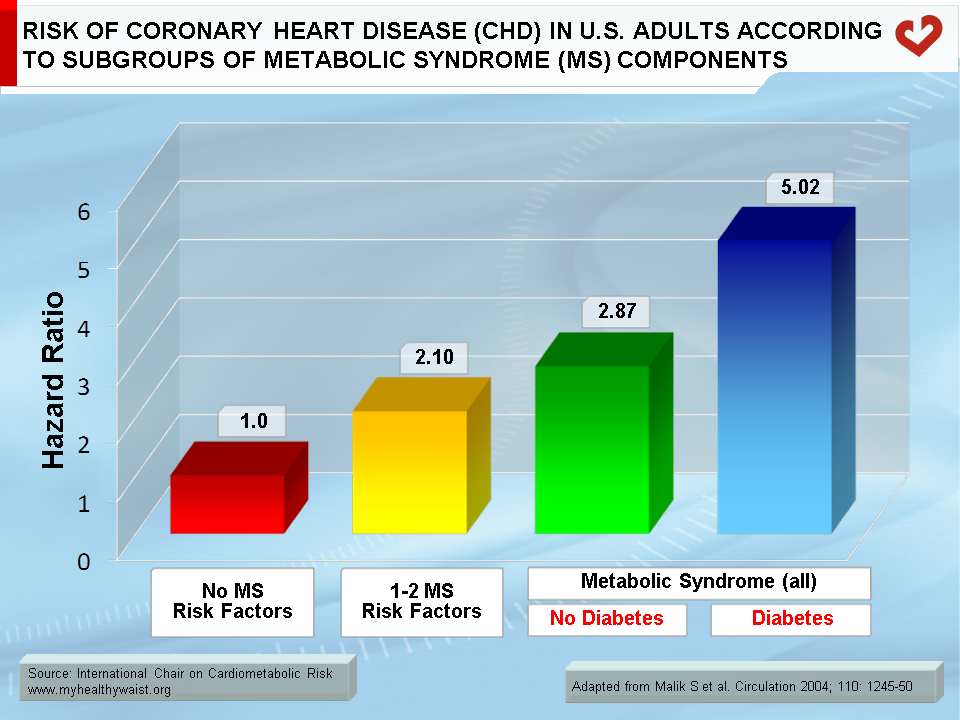
It has been suggested that individuals with even 1 or 2 metabolic syndrome risk factors are at increased risk of mortality from coronary heart disease (CHD) and CVD. However, a large prospective study from the Second National Health and Nutrition Examination Survey (NHANES II) [20] lent further support to the notion that the metabolic syndrome more strongly predicted CHD, CVD, and total mortality than its individual components alone (Figure 2), confirming previous findings [21].
Age
A major population-based retrospective cohort study [22] of 379,003 diabetic patients and 9,018,082 non-diabetic individuals showed that for both men and women, diabetes conferred a degree of risk equal to ageing roughly 15 years. Age also appeared to be an important predictor of CVD in people with diabetes, with CVD risk rising in the late 40s for both men and women. Moreover, diabetes greatly attenuated the usual protective effect enjoyed by women, narrowing the relative gender gap in cardiovascular risk [23]. Age should therefore be taken into account when aiming to reduce CVD risk in people with diabetes.
Preventing Type 2 Diabetes
It behoves those involved in treating diabetes or its complications to recognize that weight loss is the best way to prevent type 2 diabetes in overweight and obese subjects with impaired glucose tolerance. Many clinicians remain very much focused on improving glycemic control and blood lipids rather than inducing weight loss, and few diabetic clinics provide treatment or support that truly focuses on weight management. More holistic approaches to treating diabetes are needed, including one that does not only rely on expensive drugs to treat each dysmetabolic component. Effective weight management interventions should be initiated as soon as diabetes—or even pre-diabetic states such as impaired glucose tolerance or abdominal obesity—are diagnosed. The term “diabesity” has been coined because it reflects both etiology and clinical presentation. Its use could help ensure that excess body fat (abdominal obesity in particular) takes its rightful place as the major cause of type 2 diabetes [24].
References
-
Després JP and Lemieux I. Abdominal obesity and metabolic syndrome. Nature 2006; 444: 881-7
PubMed ID: 17167477
-
Lakka HM, Laaksonen DE, Lakka TA, et al. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA 2002; 288: 2709-16.
PubMed ID: 12460094
-
Gasteyger C and Tremblay A. Metabolic impact of body fat distribution. J Endocrinol Invest 2002; 25: 876-83.
PubMed ID: 12508950
-
Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001; 285: 2486-97.
PubMed ID: 11368702
-
Lemieux I, Pascot A, Couillard C, et al. Hypertriglyceridemic waist: A marker of the atherogenic metabolic triad (hyperinsulinemia; hyperapolipoprotein B; small, dense LDL) in men? Circulation 2000; 102: 179-84.
PubMed ID: 10889128
-
Palaniappan L, Carnethon MR, Wang Y, et al. Predictors of the incident metabolic syndrome in adults: the Insulin Resistance Atherosclerosis Study. Diabetes Care 2004; 27: 788-93.
PubMed ID: 14988303
-
Bergstrom RW, Newell-Morris LL, Leonetti DL, et al. Association of elevated fasting C-peptide level and increased intra-abdominal fat distribution with development of NIDDM in Japanese-American men. Diabetes 1990; 39: 104-11.
PubMed ID: 2210052
-
Lean ME, Powrie JK, Anderson AS, et al. Obesity, weight loss and prognosis in type 2 diabetes. Diabet Med 1990; 7: 228-33.
PubMed ID: 2139394
-
Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002; 346: 393-403.
PubMed ID: 11832527
-
Tuomilehto J, Lindstrom J, Eriksson JG, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med 2001; 344: 1343-50.
PubMed ID: 11333990
-
Reaven GM. The metabolic syndrome: is this diagnosis necessary? Am J Clin Nutr 2006; 83: 1237-47.
PubMed ID: 16762930
-
Meigs JB, Rutter MK, Sullivan LM, et al. Impact of insulin resistance on risk of type 2 diabetes and cardiovascular disease in people with metabolic syndrome. Diabetes Care 2007; 30: 1219-25.
PubMed ID: 17259468
-
Dekker JM, Girman C, Rhodes T, et al. Metabolic syndrome and 10-year cardiovascular disease risk in the Hoorn Study. Circulation 2005; 112: 666-73.
PubMed ID: 16061755
-
Hanley AJ, Karter AJ, Williams K, et al. Prediction of type 2 diabetes mellitus with alternative definitions of the metabolic syndrome: the Insulin Resistance Atherosclerosis Study. Circulation 2005; 112: 3713-21.
PubMed ID: 16344402
-
Rutter MK, Meigs JB, Sullivan LM, et al. Insulin resistance, the metabolic syndrome, and incident cardiovascular events in the Framingham Offspring Study. Diabetes 2005; 54: 3252-7.
PubMed ID: 16249452
-
Haffner SM and Miettinen H. Insulin resistance implications for type II diabetes mellitus and coronary heart disease. Am J Med 1997; 103: 152-62.
PubMed ID: 9274899
-
Drexel H, Aczel S, Marte T, et al. Is atherosclerosis in diabetes and impaired fasting glucose driven by elevated LDL cholesterol or by decreased HDL cholesterol? Diabetes Care 2005; 28: 101-7
PubMed ID: 15616241
-
Garg A and Grundy SM. Management of dyslipidemia in NIDDM. Diabetes Care 1990; 13: 153-69.
PubMed ID: 2190770
-
Marks JB and Raskin P. Cardiovascular risk in diabetes: a brief review. J Diabetes Complications 2000; 14: 108-15.
PubMed ID: 10959073
-
Malik S, Wong ND, Franklin SS, et al. Impact of the metabolic syndrome on mortality from coronary heart disease, cardiovascular disease, and all causes in United States adults. Circulation 2004; 110: 1245-50.
PubMed ID: 15326067
-
Isomaa B, Almgren P, Tuomi T, et al. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care 2001; 24: 683-9.
PubMed ID: 11315831
-
Booth GL, Kapral MK, Fung K, et al. Relation between age and cardiovascular disease in men and women with diabetes compared with non-diabetic people: a population-based retrospective cohort study. Lancet 2006; 368: 29-36.
PubMed ID: 16815377
-
Price JF and Fowkes FG. Risk factors and the sex differential in coronary artery disease. Epidemiology 1997; 8: 584-91.
PubMed ID: 9270963
-
Astrup A and Finer N. Redefining type 2 diabetes: ‘diabesity’ or ‘obesity dependent diabetes mellitus’? Obes Rev 2000; 1: 57-9.
PubMed ID: 12119987
 CLOSE
CLOSE
Després JP and Lemieux I. Abdominal obesity and metabolic syndrome. Nature 2006; 444: 881-7
PubMed ID: 17167477CLOSE
Lakka HM, Laaksonen DE, Lakka TA, et al. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA 2002; 288: 2709-16.
PubMed ID: 12460094CLOSE
Gasteyger C and Tremblay A. Metabolic impact of body fat distribution. J Endocrinol Invest 2002; 25: 876-83.
PubMed ID: 12508950CLOSE
Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001; 285: 2486-97.
PubMed ID: 11368702CLOSE
Lemieux I, Pascot A, Couillard C, et al. Hypertriglyceridemic waist: A marker of the atherogenic metabolic triad (hyperinsulinemia; hyperapolipoprotein B; small, dense LDL) in men? Circulation 2000; 102: 179-84.
PubMed ID: 10889128CLOSE
Palaniappan L, Carnethon MR, Wang Y, et al. Predictors of the incident metabolic syndrome in adults: the Insulin Resistance Atherosclerosis Study. Diabetes Care 2004; 27: 788-93.
PubMed ID: 14988303CLOSE
Bergstrom RW, Newell-Morris LL, Leonetti DL, et al. Association of elevated fasting C-peptide level and increased intra-abdominal fat distribution with development of NIDDM in Japanese-American men. Diabetes 1990; 39: 104-11.
PubMed ID: 2210052CLOSE
Lean ME, Powrie JK, Anderson AS, et al. Obesity, weight loss and prognosis in type 2 diabetes. Diabet Med 1990; 7: 228-33.
PubMed ID: 2139394CLOSE
Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002; 346: 393-403.
PubMed ID: 11832527CLOSE
Tuomilehto J, Lindstrom J, Eriksson JG, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med 2001; 344: 1343-50.
PubMed ID: 11333990CLOSE
Reaven GM. The metabolic syndrome: is this diagnosis necessary? Am J Clin Nutr 2006; 83: 1237-47.
PubMed ID: 16762930CLOSE
Meigs JB, Rutter MK, Sullivan LM, et al. Impact of insulin resistance on risk of type 2 diabetes and cardiovascular disease in people with metabolic syndrome. Diabetes Care 2007; 30: 1219-25.
PubMed ID: 17259468CLOSE
Dekker JM, Girman C, Rhodes T, et al. Metabolic syndrome and 10-year cardiovascular disease risk in the Hoorn Study. Circulation 2005; 112: 666-73.
PubMed ID: 16061755CLOSE
Hanley AJ, Karter AJ, Williams K, et al. Prediction of type 2 diabetes mellitus with alternative definitions of the metabolic syndrome: the Insulin Resistance Atherosclerosis Study. Circulation 2005; 112: 3713-21.
PubMed ID: 16344402CLOSE
Rutter MK, Meigs JB, Sullivan LM, et al. Insulin resistance, the metabolic syndrome, and incident cardiovascular events in the Framingham Offspring Study. Diabetes 2005; 54: 3252-7.
PubMed ID: 16249452CLOSE
Haffner SM and Miettinen H. Insulin resistance implications for type II diabetes mellitus and coronary heart disease. Am J Med 1997; 103: 152-62.
PubMed ID: 9274899CLOSE
Drexel H, Aczel S, Marte T, et al. Is atherosclerosis in diabetes and impaired fasting glucose driven by elevated LDL cholesterol or by decreased HDL cholesterol? Diabetes Care 2005; 28: 101-7
PubMed ID: 15616241CLOSE
Garg A and Grundy SM. Management of dyslipidemia in NIDDM. Diabetes Care 1990; 13: 153-69.
PubMed ID: 2190770CLOSE
Marks JB and Raskin P. Cardiovascular risk in diabetes: a brief review. J Diabetes Complications 2000; 14: 108-15.
PubMed ID: 10959073CLOSE
Malik S, Wong ND, Franklin SS, et al. Impact of the metabolic syndrome on mortality from coronary heart disease, cardiovascular disease, and all causes in United States adults. Circulation 2004; 110: 1245-50.
PubMed ID: 15326067CLOSE
Isomaa B, Almgren P, Tuomi T, et al. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care 2001; 24: 683-9.
PubMed ID: 11315831CLOSE
Booth GL, Kapral MK, Fung K, et al. Relation between age and cardiovascular disease in men and women with diabetes compared with non-diabetic people: a population-based retrospective cohort study. Lancet 2006; 368: 29-36.
PubMed ID: 16815377CLOSE
Price JF and Fowkes FG. Risk factors and the sex differential in coronary artery disease. Epidemiology 1997; 8: 584-91.
PubMed ID: 9270963CLOSE
Astrup A and Finer N. Redefining type 2 diabetes: ‘diabesity’ or ‘obesity dependent diabetes mellitus’? Obes Rev 2000; 1: 57-9.
PubMed ID: 12119987