The Epidemiological Evidence
Defining CMR - The Obesity and Type 2 Diabetes EpidemicsKey Points
- Obesity and type 2 diabetes are major cardiovascular risk factors that have reached epidemic proportions. Both diseases are increasing all over the world.
- The “diabesity” epidemic strikes all sexes, all ages, all educational levels, and all ethnicities.
- In 2016, more than 1.9 billion adults (18 years and older) were overweight and 650 million of them were obese.
- The number of diabetic individuals (20-79 years) in 2019 was 463 million. This number is expected to hit 700 million in 2045.
- Obesity and diabetes rates have increased dramatically in children and adolescents worldwide.
The Diabesity Epidemic: a Growing Burden
Among well-established cardiovascular risk factors, obesity and diabetes are on the rise [1,2]. The coronary heart disease mortality risk of diabetic patients without previous cardiovascular complications has been shown to be similar to that of nondiabetic patients who previously had a myocardial infarction [3]. This suggests that cardiovascular risk factors and complications should be treated aggressively in diabetic patients, who should be seen as post-myocardial infarction patients from a global cardiovascular disease risk standpoint [3]. Moreover, obesity—abdominal obesity in particular—is one of the major risk factors for diabetes along with physical inactivity and family history [3, 4]. To illustrate the consequences of obesity, Allison et al. [5] used data from five large cohort studies to estimate annual obesity-related deaths among U.S. adults. They estimated that obesity was a factor in approximately 280,000 deaths per year and that more than 80% of these deaths occurred among persons with a body mass index (BMI) superior to 30 kg/m2.
Shafrir [6] coined the term “diabesity” 10 years ago to illustrate the close relationship between obesity and diabetes. Both diseases share common causes, including lack of exercise and low energy expenditure combined with an unhealthy diet high in fat and refined sugar. The increasing prevalence of obesity and diabetes worldwide is a major public health threat and fighting this two-pronged epidemic will certainly be one of the biggest challenges for health professionals and our society in coming decades. This epidemic is expected to have serious health and economic consequences as obesity and diabetes rates continue to soar [7]. Obese and diabetic patients are more likely to be hospitalized for cardiovascular complications and other diabetes-related problems, such as microvascular complications, than normal weight, nondiabetic individuals.
The International Diabetes Federation (IDF) has reported that the annual global health expenditure related to diabetes is estimated to be US$760 billion. These direct costs will reach US$845 billion by 2045.
The World Health Organization (WHO) has estimated that at least 1.9 billion adults (18 years and older) worldwide were overweight in 2016, with 650 million of them being clinically obese [8]. The WHO has also reported that more than 340 million children and adolescents (5-19 years) were overweight and obese in 2019 [8]. Although the respective prevalence of obesity and diabetes is higher in western societies, these cardiovascular risk factors are rising dramatically in developing countries [2,9]. For example, in India’s fast-expanding urban centres, diabetes rates are double those in the United States [10]. Moreover, certain populations such as the Wanigela people of Papua New Guinea and the Pima Indians in Arizona are very susceptible to obesity and type 2 diabetes [11,12]. The following section provides epidemiological evidence of the obesity and diabetes epidemic that is currently sweeping the world.
Prevalence of Obesity
Though obesity is increasing rapidly in almost every part of the world, overweight and obesity rates are higher in the United States than in any other developed country [13]. A report from the National Health and Nutrition Examination Survey (NHANES)—which examined a nationally representative sample of the U.S. population—revealed that more than two thirds of the adult population (>20 years) was either overweight (BMI>25 kg/m2) or obese (BMI>30 kg/m2) [1]. The sample included 4,431 adults and showed that overweight/obesity was higher in men (70.8 ± 1.4%) than in women (51.7 ± 2.6%). The highest prevalence of overweight/obesity was among men 40 to 50 years of age (78.2 ± 2.8%). The prevalence of overweight/obesity in women in this age subgroup was 68.1 ± 3.1%. The sample was also analyzed according to ethnicity (non-Hispanic whites, non-Hispanic blacks, and Mexican Americans). The highest rates of overweight/obesity were found in the non-Hispanic black population (76.1 ± 1.5%) and among Mexican Americans (75.8 ± 2.6%). This prevalence was 64.2 ± 1.6% in the non-Hispanic white population. When these results were compared to previous results from the 1999 NHANES survey, it was found that obesity among men had increased significantly between 1999 and 2004 whereas obesity among women had not increased over the same 6-year period [1]. The study also made the unfortunate finding that obesity is increasing in children and adolescents 2 to 19 years of age, noting that 17.1 ± 1.2% of them had excess body weight.
In 1998, Flegal et al. [14] from the National Center for Health Statistics and Centers for Disease Control and Prevention (CDC) examined four different NHANES surveys (NHES I; 1960-62, NHANES I; 1971-74, NHANES II; 1976-80, and NHANES III; 1988-94). They reported a considerable increase in both overweight and obesity among adults in the United States. An 8.0% increase in obesity (BMI ≥ 30.0 kg/m2) was observed primarily between the NHANES II and III surveys (men and women 20 to 79 years of age, including all ethnic groups studied). The study also found that class III obesity prevalence (BMI ≥ 40.0 kg/m2) was over 10% among non-Hispanic black women in the middle-aged groups. In addition, the authors noted that the prevalence of non-obese overweight (BMI 25.0-29.9 kg/m2) was higher in men than in women, the prevalence of class I obesity (BMI 30.0-34.9 kg/m2) was similar in both genders, and more women than men had a BMI ≥ 35.0 kg/m2 [14].
Another study using data from NHANES surveys has suggested that obesity is associated with excess deaths in the United States [15]. The strongest association between elevated body weight and mortality was observed in men and women 25 to 59 years of age who had a BMI ≥ 35 kg/m2 and a relative risk of overall mortality of 1.83 (95% CI, 1.27-2.62) compared to the normal weight category. This study also highlighted that the association between excess body weight and mortality was stronger in NHANES I than in NHANES III, suggesting that public health and medical care improvements may be weakening the ties between elevated BMI and mortality. To illustrate the growing obesity epidemic, Figure 1 shows the increase in overweight and obesity rates in U.S. children and adults from 1960 to 2000.
Other affluent countries such as the United Kingdom have also experienced a sharp jump in obesity in recent decades. The Health Survey for England indicated that obesity rose threefold between 1980 and 2002. In 1980, 6% of men and 8% of women were obese. In 2002, these figures reached 23% for men and 25% for women. Like most other Western countries, obesity tended to increase with age (up to 64 years), be higher in people with low income or low education, and show an upward trend in children and adolescents, suggesting that obesity rates in young adults are sure to rise in coming years [16].
Obesity rates are lower in Scandinavian countries than in other developed societies. Yet obesity rates are also on the rise in this part of the world as well. According to the Survey of Living Conditions, obesity doubled in Swedish men and women aged 16 to 84 between 1980-1981 and 2002-2003 [17]. Overweight and obesity rates increased dramatically between 1971 and 1995. Hardest hit were 18-year-old boys. For them, the prevalence of overweight doubled to 16.3% and the prevalence of obesity almost quadrupled to 3.2% [18].
China is a good example of how the growing obesity epidemic takes root in countries moving to a capitalist, free market economy. China is the world’s most populated country with one-fifth of the world’s population. The country’s economy is growing exponentially with the per capita gross domestic product increasing tenfold between 1982 and 2000 [19].
Over the last few decades, the Chinese population has become more sedentary, more urbanized, and increasingly reliant on cars and high-calorie, energy-dense food. These cultural and behavioural changes have had a considerable impact on Chinese obesity rates. A meta-analysis by Wang et al. [19] reported that, between 1992 and 2002, obesity and overweight increased in both sexes, in all age groups, and in all geographic areas. According to the WHO classification of obesity and overweight, the percentage of obese and overweight Chinese adults—which was 14.6% in 1992—has now increased to 21.8%. Although rates of obesity and overweight are somewhat lower than in the United States, the striking increase in obesity and overweight in China combined with the fact that this population is more prone to diabetes than Caucasians could mean that a dramatic spike in Chinese diabetes rates is just around the corner. Chinese urban residents are more likely to be overweight and obese. In 2002, according to Chinese standards of overweight (24 ≤ BMI < 28 kg/m2) and obesity (BMI ≥ 28 kg/m2), 35.1% of Beijing adults were overweight and 20.6% were obese. In addition to showing that overweight and obesity had increased 50% in the last decade, the study also highlighted significant changes to mortality and morbidity patterns in China. Though infectious diseases dropped sharply, there was an increase in chronic diseases related to excess body weight, such as hypertension, cardiovascular disease, and type 2 diabetes [19].

Childhood Obesity
The global diabesity epidemic and its related comorbidities have now attacked children and adolescents all over the world. Maternal and paternal obesity, a sedentary lifestyle, and low birth weight are all risk factors tied to excess body weight in youth [20]. According to the WHO, the prevalence of overweight and obesity among children and adolescents (5-19 years) increased from 4% in 1975 to more than 18% in 2016 [8]. NHANES evaluated the prevalence of childhood obesity in the U.S. between 1976 and 2002 and found that overweight and obesity rates went from 4% to 6% between 1976 and 1980 and reached 16% in 2002 [21].
Obesity is also closely tied to impaired glucose tolerance and type 2 diabetes in children and adolescents. Although type 1 diabetes is the most common chronic disease in children, type 2 diabetes is expected to overtake type 1 diabetes in the near future [22]. Similarly, clinical manifestations of type 2 diabetes are now being observed at a very young age. In the U.S., Arslanian et al. [23] have estimated that type 2 diabetes is diagnosed in approximately 20% of pubertal children referred to diabetes clinics. A number of developing countries in Latin America, the Caribbean, the Middle East, and North Africa are also facing an obesity epidemic in preschool children [24].
Prevalence of Diabetes
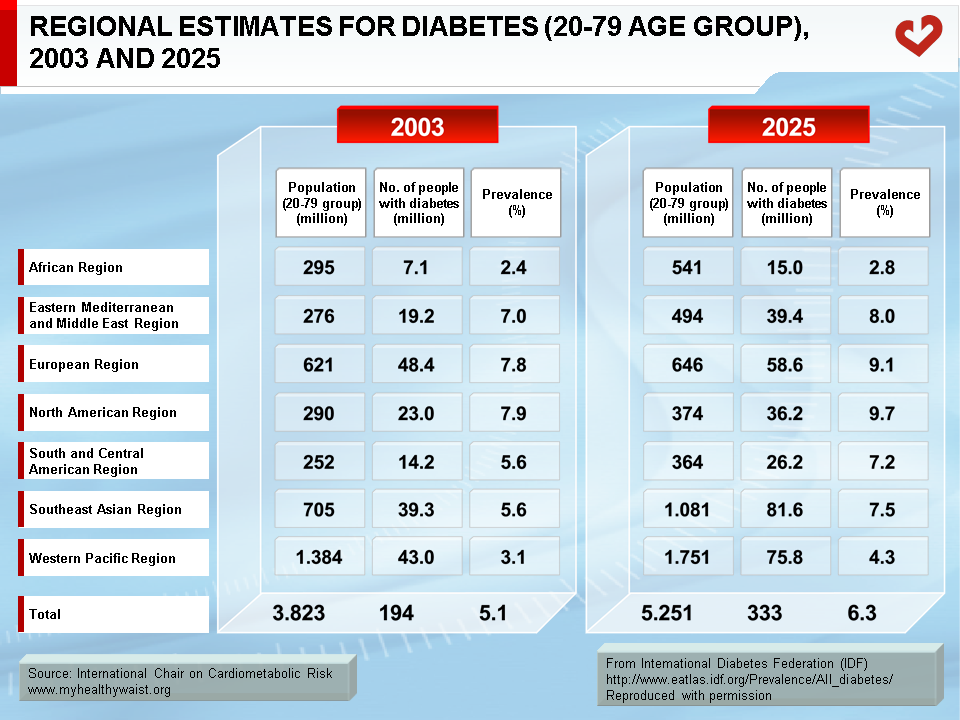
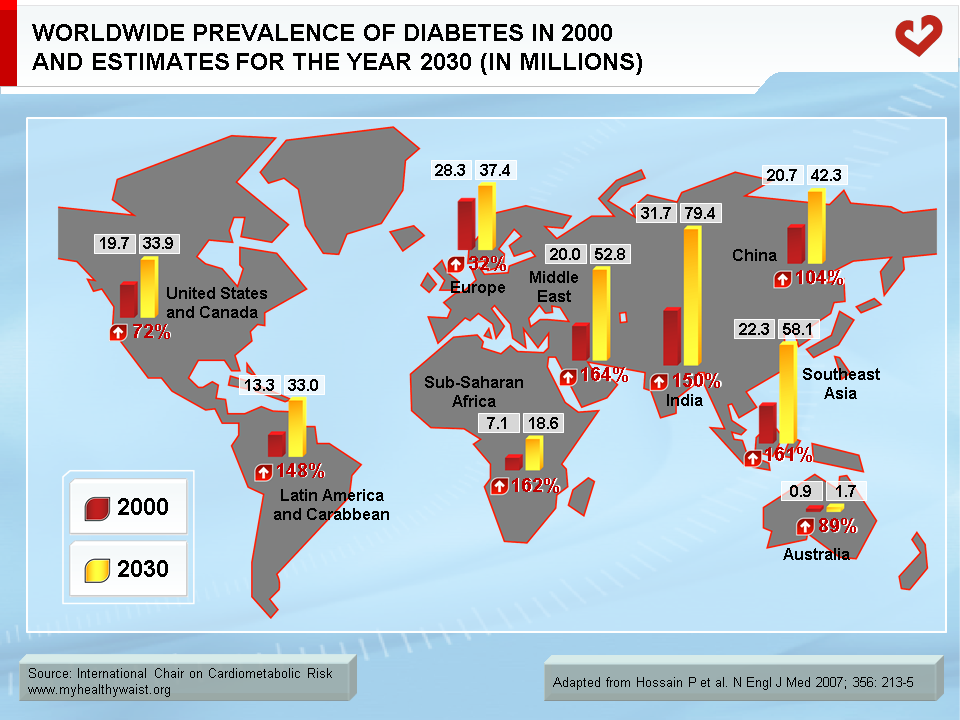
Diabetes is now considered to be the 7th leading cause of death worldwide after ischemic heart disease, stroke, chronic obstructive pulmonary disease, lower respiratory infections, Alzheimer disease and other dementias; and trachea, bronchus and lung cancers [25]. Similar to those for obesity, risk factors for type 2 diabetes include age, family history of type 2 diabetes (or obesity), impaired glucose metabolism, physical inactivity, and ethnicity. Obesity is also a major modifiable risk factor for type 2 diabetes [3]. It has been proposed that between 60% and 90% of type 2 diabetes cases are due to excess body weight [26]. Worldwide, 177 million individuals were considered to be diabetic in 2000 and some 90-95% of them had type 2 diabetes [27]. According to the CDC, nearly 21 million Americans have diabetes. The CDC has also reported that among those 20 and over, 8.7% of non-Hispanic whites, 13.3% of non-Hispanic blacks, and 9.5% of Hispanic/Latino Americans have diabetes. Non-Hispanic blacks are 1.8 times more likely to develop diabetes than non-Hispanic whites. It has been estimated that, in 2000, excess mortality due to diabetes accounted for over 8% of deaths in Western societies such as the U.S. and Canada and for 2-3% of deaths in poorer countries [28]. Although diabetes rates are lower in developing countries, rates are shooting up in the Middle East, Pacific Islands, Southeast Asia, and China, especially in urban areas (Table). To illustrate diabetes’ global reach and the continuing type 2 diabetes epidemic, Figure 2 depicts the prevalence of diabetes in many parts of the world along with projected percent changes up to the year 2030 as estimated by Wild et al. [29]. For example, the number of diabetic individuals in India is expected to increase threefold between 2000 and 2030.
Moreover, even if obesity rates stabilize during this period (which is very unlikely to happen), the number of people with diabetes worldwide would still double because of urbanization, aging, and improved survival [30].
In summary, sweeping public health measures should be implemented throughout the world to counter the diabesity epidemic. These measures should encourage all people to take part in regular physical activity, regardless of their age, sex, or social class. In preventing obesity and obesity-related diabetes, special emphasis should also be placed on improving the nutritional habits of at-risk individuals and the general population, who are likely to eat energy-dense diets. According to the IDF, up to 80% of type 2 diabetes cases can be prevented by adopting a healthy diet and increasing physical activity. It is equally important to diagnose type 2 diabetes since over 50% of type 2 diabetes sufferers around the world are unaware of their condition.
References
-
Ogden CL, Carroll MD, Curtin LR, et al. Prevalence of overweight and obesity in the United States, 1999-2004. JAMA 2006; 295: 1549-55.
PubMed ID: 16595758
-
Zimmet P, Alberti KG and Shaw J. Global and societal implications of the diabetes epidemic. Nature 2001; 414: 782-7.
PubMed ID: 11742409
-
Haffner SM. Epidemiology of type 2 diabetes: risk factors. Diabetes Care 1998; 21 Suppl 3: C3-6.
PubMed ID: 9850478
-
Ekelund U, Griffin SJ and Wareham NJ. Physical activity and metabolic risk in individuals with a family history of type 2 diabetes. Diabetes Care 2007; 30: 337-42.
PubMed ID: 17259504
-
Allison DB, Fontaine KR, Manson JE, et al. Annual deaths attributable to obesity in the United States. JAMA 1999; 282: 1530-8.
PubMed ID: 10546692
-
Shafrir E. Development and consequences of insulin resistance: lessons from animals with hyperinsulinaemia. Diabetes Metab 1996; 22: 122-31.
PubMed ID: 8792092
-
Smyth S and Heron A. Diabetes and obesity: the twin epidemics. Nat Med 2006; 12: 75-80.
PubMed ID: 16397575
-
World Health Organization. Obesity and overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
PubMed ID:
-
Mendis S, Yach D, Bengoa R, et al. Research gap in cardiovascular disease in developing countries. Lancet 2003; 361: 2246-7.
PubMed ID: 12842389
-
Dirks JH, Robinson SW, Alderman M, et al. Meeting report on the Bellagio Conference ‘prevention of vascular diseases in the emerging world: An approach to global health equity’. Kidney Int 2006; 70: 1397-402.
PubMed ID: 16955109
-
Dowse GK, Spark RA, Mavo B, et al. Extraordinary prevalence of non-insulin-dependent diabetes mellitus and bimodal plasma glucose distribution in the Wanigela people of Papua New Guinea. Med J Aust 1994; 160: 767-74.
PubMed ID: 8208193
-
Bennett PH, Burch TA and Miller M. Diabetes mellitus in American (Pima) Indians. Lancet 1971; 2: 125-8.
PubMed ID: 4104461
-
Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser 2000; 894: i-xii, 1-253.
PubMed ID: 11234459
-
Flegal KM, Carroll MD, Kuczmarski RJ, et al. Overweight and obesity in the United States: prevalence and trends, 1960-1994. Int J Obes Relat Metab Disord 1998; 22: 39-47.
PubMed ID: 9481598
-
Flegal KM, Graubard BI, Williamson DF, et al. Excess deaths associated with underweight, overweight, and obesity. JAMA 2005; 293: 1861-7.
PubMed ID: 15840860
-
Rennie KL and Jebb SA. Prevalence of obesity in Great Britain. Obes Rev 2005; 6: 11-2.
PubMed ID: 15655034
-
Sundquist K, Qvist J, Johansson SE, et al. Increasing trends of obesity in Sweden between 1996/97 and 2000/01. Int J Obes Relat Metab Disord 2004; 28: 254-61.
PubMed ID: 14647184
-
Rasmussen F and Johansson M. Increase in the prevalence of overweight and obesity from 1995 to 1998 among 18-year-old males in Sweden. Acta Paediatr 2000; 89: 888-9.
PubMed ID: 10943978
-
Wang Y, Mi J, Shan XY, et al. Is China facing an obesity epidemic and the consequences? The trends in obesity and chronic disease in China. Int J Obes (Lond) 2007; 31: 177-88.
PubMed ID: 16652128
-
Celermajer DS and Ayer JG. Childhood risk factors for adult cardiovascular disease and primary prevention in childhood. Heart 2006; 92: 1701-6.
PubMed ID: 17041125
-
Ogden CL, Flegal KM, Carroll MD, et al. Prevalence and trends in overweight among US children and adolescents, 1999-2000. JAMA 2002; 288: 1728-32.
PubMed ID: 12365956
-
Fagot-Campagna A, Pettitt DJ, Engelgau MM, et al. Type 2 diabetes among North American children and adolescents: an epidemiologic review and a public health perspective. J Pediatr 2000; 136: 664-72.
PubMed ID: 10802501
-
Arslanian S. Type 2 diabetes in children: clinical aspects and risk factors. Horm Res 2002; 57 Suppl 1: 19-28.
PubMed ID: 11979018
-
Martorell R, Kettel Khan L, Hughes ML, et al. Overweight and obesity in preschool children from developing countries. Int J Obes Relat Metab Disord 2000; 24: 959-67.
PubMed ID: 10951533
-
World Health Organization. The top 10 causes of death. https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death
PubMed ID:
-
Stumvoll M, Goldstein BJ and van Haeften TW. Type 2 diabetes: principles of pathogenesis and therapy. Lancet 2005; 365: 1333-46.
PubMed ID: 15823385
-
Amos AF, McCarty DJ and Zimmet P. The rising global burden of diabetes and its complications: estimates and projections to the year 2010. Diabet Med 1997; 14 Suppl 5: S1-85.
PubMed ID: 9450510
-
Roglic G, Unwin N, Bennett PH, et al. The burden of mortality attributable to diabetes: realistic estimates for the year 2000. Diabetes Care 2005; 28: 2130-5.
PubMed ID: 16123478
-
Wild S, Roglic G, Green A, et al. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 2004; 27: 1047-53.
PubMed ID: 15111519
-
Hossain P, Kawar B and El Nahas M. Obesity and diabetes in the developing world–a growing challenge. N Engl J Med 2007; 356: 213-5.
PubMed ID: 17229948
 CLOSE
CLOSE
Ogden CL, Carroll MD, Curtin LR, et al. Prevalence of overweight and obesity in the United States, 1999-2004. JAMA 2006; 295: 1549-55.
PubMed ID: 16595758CLOSE
Zimmet P, Alberti KG and Shaw J. Global and societal implications of the diabetes epidemic. Nature 2001; 414: 782-7.
PubMed ID: 11742409CLOSE
Haffner SM. Epidemiology of type 2 diabetes: risk factors. Diabetes Care 1998; 21 Suppl 3: C3-6.
PubMed ID: 9850478CLOSE
Ekelund U, Griffin SJ and Wareham NJ. Physical activity and metabolic risk in individuals with a family history of type 2 diabetes. Diabetes Care 2007; 30: 337-42.
PubMed ID: 17259504CLOSE
Allison DB, Fontaine KR, Manson JE, et al. Annual deaths attributable to obesity in the United States. JAMA 1999; 282: 1530-8.
PubMed ID: 10546692CLOSE
Shafrir E. Development and consequences of insulin resistance: lessons from animals with hyperinsulinaemia. Diabetes Metab 1996; 22: 122-31.
PubMed ID: 8792092CLOSE
Smyth S and Heron A. Diabetes and obesity: the twin epidemics. Nat Med 2006; 12: 75-80.
PubMed ID: 16397575CLOSE
World Health Organization. Obesity and overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
PubMed ID:CLOSE
Mendis S, Yach D, Bengoa R, et al. Research gap in cardiovascular disease in developing countries. Lancet 2003; 361: 2246-7.
PubMed ID: 12842389CLOSE
Dirks JH, Robinson SW, Alderman M, et al. Meeting report on the Bellagio Conference ‘prevention of vascular diseases in the emerging world: An approach to global health equity’. Kidney Int 2006; 70: 1397-402.
PubMed ID: 16955109CLOSE
Dowse GK, Spark RA, Mavo B, et al. Extraordinary prevalence of non-insulin-dependent diabetes mellitus and bimodal plasma glucose distribution in the Wanigela people of Papua New Guinea. Med J Aust 1994; 160: 767-74.
PubMed ID: 8208193CLOSE
Bennett PH, Burch TA and Miller M. Diabetes mellitus in American (Pima) Indians. Lancet 1971; 2: 125-8.
PubMed ID: 4104461CLOSE
Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser 2000; 894: i-xii, 1-253.
PubMed ID: 11234459CLOSE
Flegal KM, Carroll MD, Kuczmarski RJ, et al. Overweight and obesity in the United States: prevalence and trends, 1960-1994. Int J Obes Relat Metab Disord 1998; 22: 39-47.
PubMed ID: 9481598CLOSE
Flegal KM, Graubard BI, Williamson DF, et al. Excess deaths associated with underweight, overweight, and obesity. JAMA 2005; 293: 1861-7.
PubMed ID: 15840860CLOSE
Rennie KL and Jebb SA. Prevalence of obesity in Great Britain. Obes Rev 2005; 6: 11-2.
PubMed ID: 15655034CLOSE
Sundquist K, Qvist J, Johansson SE, et al. Increasing trends of obesity in Sweden between 1996/97 and 2000/01. Int J Obes Relat Metab Disord 2004; 28: 254-61.
PubMed ID: 14647184CLOSE
Rasmussen F and Johansson M. Increase in the prevalence of overweight and obesity from 1995 to 1998 among 18-year-old males in Sweden. Acta Paediatr 2000; 89: 888-9.
PubMed ID: 10943978CLOSE
Wang Y, Mi J, Shan XY, et al. Is China facing an obesity epidemic and the consequences? The trends in obesity and chronic disease in China. Int J Obes (Lond) 2007; 31: 177-88.
PubMed ID: 16652128CLOSE
Celermajer DS and Ayer JG. Childhood risk factors for adult cardiovascular disease and primary prevention in childhood. Heart 2006; 92: 1701-6.
PubMed ID: 17041125CLOSE
Ogden CL, Flegal KM, Carroll MD, et al. Prevalence and trends in overweight among US children and adolescents, 1999-2000. JAMA 2002; 288: 1728-32.
PubMed ID: 12365956CLOSE
Fagot-Campagna A, Pettitt DJ, Engelgau MM, et al. Type 2 diabetes among North American children and adolescents: an epidemiologic review and a public health perspective. J Pediatr 2000; 136: 664-72.
PubMed ID: 10802501CLOSE
Arslanian S. Type 2 diabetes in children: clinical aspects and risk factors. Horm Res 2002; 57 Suppl 1: 19-28.
PubMed ID: 11979018CLOSE
Martorell R, Kettel Khan L, Hughes ML, et al. Overweight and obesity in preschool children from developing countries. Int J Obes Relat Metab Disord 2000; 24: 959-67.
PubMed ID: 10951533CLOSE
World Health Organization. The top 10 causes of death. https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death
PubMed ID:CLOSE
Stumvoll M, Goldstein BJ and van Haeften TW. Type 2 diabetes: principles of pathogenesis and therapy. Lancet 2005; 365: 1333-46.
PubMed ID: 15823385CLOSE
Amos AF, McCarty DJ and Zimmet P. The rising global burden of diabetes and its complications: estimates and projections to the year 2010. Diabet Med 1997; 14 Suppl 5: S1-85.
PubMed ID: 9450510CLOSE
Roglic G, Unwin N, Bennett PH, et al. The burden of mortality attributable to diabetes: realistic estimates for the year 2000. Diabetes Care 2005; 28: 2130-5.
PubMed ID: 16123478CLOSE
Wild S, Roglic G, Green A, et al. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 2004; 27: 1047-53.
PubMed ID: 15111519CLOSE
Hossain P, Kawar B and El Nahas M. Obesity and diabetes in the developing world–a growing challenge. N Engl J Med 2007; 356: 213-5.
PubMed ID: 17229948