On numerous occasions, scientists associated with the research and educational activities of the International Chair on Cardiometabolic Risk (ICCR) have raised concerns regarding the progressive change observed in our drinking habits over the last 40 years. For instance, the consumption of milk has decreased and been progressively substituted for sugar-sweetened beverages [1]. Numerous epidemiological studies and clinical investigations have now shown that there is a relationship between the overconsumption of sugar-sweetened beverages and the risk of obesity, type 2 diabetes and cardiovascular disease [2-5]. In addition, the glycemic load associated with an overconsumption of sugar-sweetened beverages may represent a stress for the pancreatic beta cells leading to a chronic oversecretion of insulin [2]. Over the long term, this may contribute to beta cell exhaustion and to the progressive development of a dysglycemic state leading to type 2 diabetes. Studies have also suggested that the overconsumption of sugary drinks is not accompanied by a compensatory decrease in the intake of calories coming from solid foods [6-7]. Therefore, overconsumption of sugar-sweetened beverages may contribute to a passive excess intake of calories contributing to a positive energy balance and to the development of obesity [2, 4].
 Water has been the main source of hydration favoured by the experts of the ICCR as it contains no calories and is neutral for cardiometabolic health [8-9]. Indeed, water should be the basis of our hydration, particularly among individuals afflicted by overweight, abdominal obesity or metabolic diseases such as type 2 diabetes. However, a frequently asked question remains: Are there other safe and possibly beneficial sources of hydration for cardiometabolic health?
Water has been the main source of hydration favoured by the experts of the ICCR as it contains no calories and is neutral for cardiometabolic health [8-9]. Indeed, water should be the basis of our hydration, particularly among individuals afflicted by overweight, abdominal obesity or metabolic diseases such as type 2 diabetes. However, a frequently asked question remains: Are there other safe and possibly beneficial sources of hydration for cardiometabolic health?
Numerous studies conducted by investigators of the Harvard School of Public Health have shown that coffee consumption (not caffeine) was associated with a reduced risk of developing type 2 diabetes [10-11]. Furthermore, coffee and tea consumption do not appear to have a negative influence on the risk of cardiovascular disease [12-13] and some studies have even suggested that it may carry some protection. In addition, recent studies conducted by the team of Dr. Frank Hu, from the same institution, have shown that the American nurses who had systematically consumed dairy products from their adolescence to adulthood were at reduced risk of developing type 2 diabetes compared to low consumers of dairy products [14]. Such observation is fully concordant with other studies which have suggested that the consumption of milk and dairy products could be associated with a reduced risk of developing insulin resistance and its related atherogenic dyslipidemia and type 2 diabetes [15-18]. Additional studies will therefore be warranted in order to better understand the mechanisms by which the consumption of unsweetened coffee and tea as well as of dairy products could offer some protection against the development of cardiometabolic diseases. However, in a context where the overconsumption of sugar-sweetened beverages is on the “radar screen” of many public health organizations, these recent studies suggest that alternate options could be considered in order to offer a portfolio of hydration compatible with optimal cardiometabolic health. At the ICCR, we therefore propose an inverted pyramid of hydration where the unlimited consumption of water is favoured above all (Figure). However, the regular consumption of unsweetened coffee and tea is also allowed. Regarding dairy products, the effects on cardiometabolic health are encouraging and clearly deserve further attention. For the moment, we favour the consumption of dairy products with a low fat content. However, recent studies from Mozaffarian and colleagues [19] and other groups [20] have even suggested that the trans fatty acids specifically derived from dairy products could have beneficial effects on features of the insulin resistance syndrome. These possibly beneficial properties will have to be confirmed by clinical studies. Meanwhile, the additional calories associated with the fat content of dairy products should also be considered until further evidence becomes available. Other components of dairy products such as calcium, magnesium, lactose and dairy proteins may also be involved and are under investigation [17].
In addition, a frequently asked question relates to the consumption of diet drinks containing no caloric sweeteners. Although they were the source of concerns, recent studies suggest that their regular consumption may not increase cardiometabolic risk per se and may not represent a safety problem [21]. We therefore consider that they could have a place in the hydration portfolio but that they should not represent the main form of hydration since compared to water, their complete safety over a lifespan is not firmly established.
Finally, fruit juices, although containing vitamins and fibres, represent an important source of sugar and calories and their consumption should be limited and preferably replaced by the consumption of fresh fruits. Therefore, at the basis of this inverted hydration pyramid we will find fruit drinks, energy drinks and sugar-sweetened beverages as they should be consumed with moderation (Figure). Indeed, the signal that we get from the scientific literature appears quite clear: Although other factors are obviously involved, the overconsumption of these sugary drinks plays a role in the development of obesity, type 2 diabetes and cardiovascular disease.
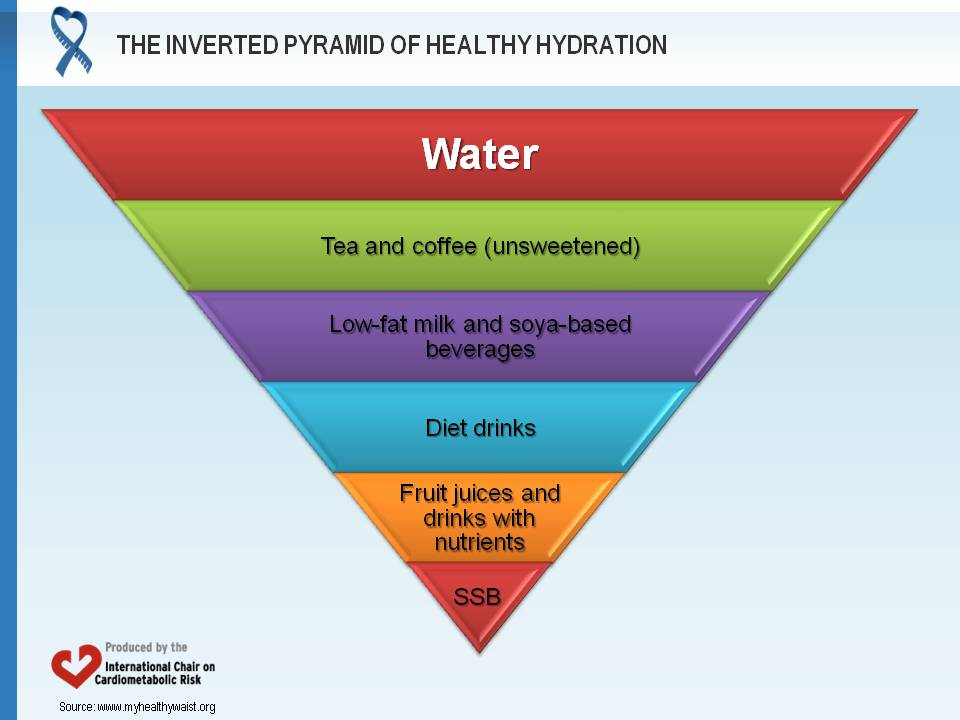
This pyramid may be further detailed or modified when additional scientific evidence (e.g. milk, diet drinks) becomes available. At the top, the consumption of water is the preferred hydration option whereas sugar-sweetened beverages (SSB) are at the bottom since their consumption should be limited. This pyramid will be particularly relevant to sedentary individuals who are abdominally obese and characterized by comorbidities such as insulin resistance, atherogenic dyslipidemia, hypertension, type 2 diabetes and cardiovascular disease. Obviously, endurance-trained athletes performing prolonged exercise may even benefit from other sources of hydration than water during very long exercise bouts. The present recommendations aim at a large segment of the population who is sedentary or only moderately active.
References
- Brownell KD, Farley T, Willett WC, et al. The public health and economic benefits of taxing sugar-sweetened beverages. N Engl J Med 2009; 361: 1599-605. PubMed ID: 19759377
- Malik VS, Popkin BM, Bray GA, et al. Sugar-sweetened beverages, obesity, type 2 diabetes mellitus, and cardiovascular disease risk. Circulation 2010; 121: 1356-64. PubMed ID: 20308626
- Malik VS, Popkin BM, Bray GA, et al. Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes: a meta-analysis. Diabetes Care 2010; 33: 2477-83. PubMed ID: 20693348
- Malik VS, Schulze MB and Hu FB. Intake of sugar-sweetened beverages and weight gain: a systematic review. Am J Clin Nutr 2006; 84: 274-88. PubMed ID: 16895873
- Fung TT, Malik V, Rexrode KM, et al. Sweetened beverage consumption and risk of coronary heart disease in women. Am J Clin Nutr 2009; 89: 1037-42. PubMed ID: 19211821
- DiMeglio DP and Mattes RD. Liquid versus solid carbohydrate: effects on food intake and body weight. Int J Obes Relat Metab Disord 2000; 24: 794-800. PubMed ID: 10878689
- Raben A, Vasilaras TH, Moller AC, et al. Sucrose compared with artificial sweeteners: different effects on ad libitum food intake and body weight after 10 wk of supplementation in overweight subjects. Am J Clin Nutr 2002; 76: 721-9. PubMed ID: 12324283
- Hu FB. Sugar-sweetened beverages as a major modifiable risk factor for type 2 diabetes. CMReJournal 2010; 3: 9-12. http://www.myhealthywaist.org/cmrejournal/articles/vol3/v3i3a3.php. Accessed March 2, 2020.
- Popkin B. Global dimensions of sugary beverages and programmatic and policy solutions. CMReJournal 2009; 2: 6-9. http://www.myhealthywaist.org/cmrejournal/pdf/vol2/v2i2a2.pdf. Accessed March 2, 2020.
- van Dam RM and Hu FB. Coffee consumption and risk of type 2 diabetes: a systematic review. JAMA 2005; 294: 97-104. PubMed ID: 15998896
- van Dam RM, Willett WC, Manson JE, et al. Coffee, caffeine, and risk of type 2 diabetes: a prospective cohort study in younger and middle-aged U.S. women. Diabetes Care 2006; 29: 398-403. PubMed ID: 16443894
- Lopez-Garcia E, Rodriguez-Artalejo F, Li TY, et al. Coffee consumption and mortality in women with cardiovascular disease. Am J Clin Nutr 2011; 94: 218-24. PubMed ID: 21562090
- Deka A and Vita JA. Tea and cardiovascular disease. Pharmacol Res 2011; 64: 136-45. PubMed ID: 21477653
- Malik VS, Sun Q, van Dam RM, et al. Adolescent dairy product consumption and risk of type 2 diabetes in middle-aged women. Am J Clin Nutr 2011; 94: 854-61. PubMed ID: 21753066
- Tong X, Dong JY, Wu ZW, et al. Dairy consumption and risk of type 2 diabetes mellitus: a meta-analysis of cohort studies. Eur J Clin Nutr 2011; 65: 1027-31. PubMed ID: 21559046
- German JB, Gibson RA, Krauss RM, et al. A reappraisal of the impact of dairy foods and milk fat on cardiovascular disease risk. Eur J Nutr 2009; 48: 191-203. PubMed ID: 19259609
- Tremblay A and Gilbert JA. Milk products, insulin resistance syndrome and type 2 diabetes. J Am Coll Nutr 2009; 28 Suppl 1: 91S-102S. PubMed ID: 19571167
- Pittas AG, Lau J, Hu FB, et al. The role of vitamin D and calcium in type 2 diabetes. A systematic review and meta-analysis. J Clin Endocrinol Metab 2007; 92: 2017-29. PubMed ID: 17389701
- Mozaffarian D, Cao H, King IB, et al. Trans-palmitoleic acid, metabolic risk factors, and new-onset diabetes in U.S. adults: a cohort study. Ann Intern Med 2010; 153: 790-9. PubMed ID: 21173413
- Motard-Bélanger A, Charest A, Grenier G, et al. Study of the effect of trans fatty acids from ruminants on blood lipids and other risk factors for cardiovascular disease. Am J Clin Nutr 2008; 87: 593-9. PubMed ID: 18326596
- American Dietetic Association. Position of the American Dietetic Association: use of nutritive and nonnutritive sweeteners. J Am Diet Assoc 2004; 104: 255-75. PubMed ID: 14760578